
Edel kindly presented this on the first Rehab In Sport webinar.
She currently leads the upper limb team at the Sport Surgery Clinic in Ireland and is completing her PHD looking at the return to sport post shoulder stabilisation. In her role at the Sport Surgery Clinic Edel sees a lot of contact athletes with traumatic instability events.
During the webinar she discussed her clinical reasoning when rehabbing the young contact athlete, the quick wins in rehab, the criteria based progressions she uses, and the objective outcomes that can be used to return to sport during a shoulder reconstruction rehabilitation.
Edel presented a return to sport case example of a 21 year old semi professional player post latarjet surgery.
The Lateajet process:
During the latarjet the surgeon sections some of the coracoid process, contours it to line up with the glenoid (socket part). These are usually performed on players with bony defect in the glenoid.
This surgery provides 3 points of stability to the shoulder by attaching the coracoid process to the glenoid, the conjoint tendon acting like a sling and the repair capsule itself.
The rehab process
Early phase
There is some debate around the sling, with times depending on the surgeon. Athletes are usually kept in a sling for 2 – 4 weeks. Elite athletes can come out earlier, around 10 days due to better supervision.
Protect the repair
There is a risk of a hematoma or infection post surgery. It is important to allow the capsule to heal.
Trauma usually only affects passive structures
The rehab in the early stage can work in a safe zone where you don’t put much strain on the repair. This is typically 20-30 degrees external rotation, 90 degree and above flexion. You can do clever stuff early on to get everything firing.
Closed chain exercises
These tend to have a lower MVC in some muscle groups, lower than actually taking the arm in and out of the sling. They are a good way in during the first 10 – 14 days to get some activation while protecting the shoulder.
Avoid muscle atrophy and cuff inhibition
Cross education
Using unilateral strength training to allow for some contralateral crossover to preserve muscle size and strength in the immobilized limb.
6 weeks
Edel highlighted some pitfalls and niggles seen with this cohort.
At 6 weeks post op the aim is to optimise rotational range and strength.
Reduced range of motion has potential for risk of injury, more so for overhead athletes over contact athletes.
It is an opportunity to fine tune things. You want to get the small stuff right now so when you add in the strength and power work later on you don’t want to be having pain and niggles as a result of neglecting the small stuff.
Rotational exercises and the posterior cuff (supraspinatus, infraspinatus and teres minor). There are lots of different exercises to choose from but which ones are best? How do we know what are the best ones to do? What ones can be done early on as activation and control exercises?
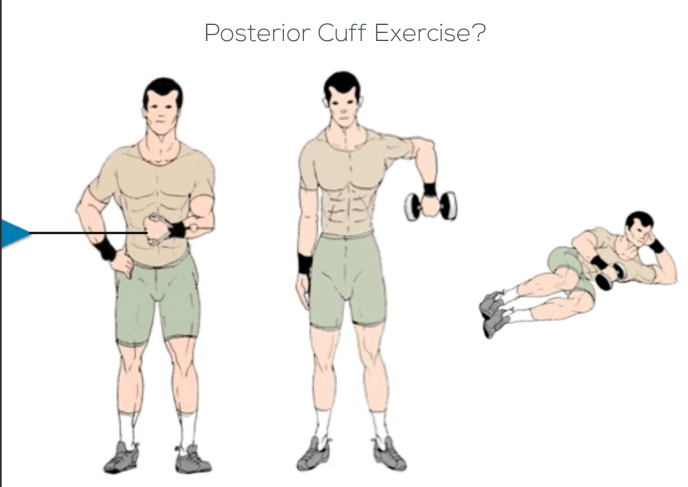
Loaded or Unloaded?
If we add more load or more theraband in to a rotation exercise does it make a difference? Are we recruiting more rotator cuff?

Just because we add more load, it doesn’t change the recruitment pattern.
Adding more load doesn’t target just the posterior cuff activity but targets everything that externally rotates.
Supported or unsupported?

Does supporting the arm change the recruitment of the posterior cuff?

The less support the shoulder gets in 90/90 position, the more recruitment you get of the rotator cuff (supraspinatus / infraspinatus).
Post surgery, these muscles groups are weak with lower muscle activity. Early on the key is to support arm to get full range of motion then start loading.
When people take the support away too early, before they have full range, they tend to end up not getting the full range back.
Support the arm to get the range then take the support away.
Working in the flexion plane is safe as it puts no strain on repair as opposed to coming out in the 90/90 position. This can be done quite early on as the arm is fully supported, allowing you to gain some control and range.
Flexion based exercises recruit the posterior cuff more than extension exercises.

Wall Step – Early activation and control exercise. Use the operated arm in the static position as this is a safe position.
Wall Walks – Progress to working through range activities
Y – Exercise – helps to tidy up flexion range. To get end range flexion you need end range external rotation, they feed in to each other.
VW – Exercise – Laterjet athletes tend to struggle with end range flexion and external rotation which can inhibit overhead pressing and pull ups.
It is important to tidy up the small stuff first to complement the strength and power work.
9 weeks
There are about 400 shoulder stabilisations at the Sport Surgery Clinic each year and the challenges at this point are gaining end range active and passive external rotation.
Working the posterior cuff with the band in to the end range, feeling the activation at the back of the cuff. Important as there can be an active lag here which feeds in to end range flexion which is important to allow catching the ball over head.
Flexion plane leads in to the scaption plane work. Focusing on time under tension at the end ranges.
Prone rotations starting supported and working to unsupported. Working in to end ranges and pulsing.
The other deficit seen at the 9 week mark (or 4 – 6 month mark if not addressed) is a deficit in the inner ranger anterior cuff (subscapularis).
A deficit in bottom of 90/90 position is a result of the surgery cutting through subscapularis. It is unusual to see an anterior cuff deficit unless there is an anterior cuff tear or Latarjet where they cut through the subscapularis.
Ginn et al 2017 have looked at the optimal exercises to strengthen subscapularis:
https://www.sciencedirect.com/science/article/abs/pii/S1440244016302341

Subscapularis activity was high across all exercises but in the belly-press (D) it was significantly higher compared to surrounding muscle groups during this exercise.

Standing rotations in neutral is a good way to get the anterior cuff switched on and keeping in the inner range, working on time under tension.
Start in neutral first before working to higher positions.
When can you add some of the push and pull work? If they have a balanced cuff in neutral then they can start doing some of the horizontal work (floor press / SA DB press). These are great exercises as they produce huge torque through the rotator cuff as long as you have a fairly stable and balanced cuff to work with.
At clubs with a lot of access to physiotherapy the athletes can start the horizontal push work from the 4 – 6 week mark if they are under pressure to return them to play, as they need time to work through the continuum of strength and power.
With the overhead vertical push work, it can often be a bit nipper if you don’t have nice control in flexion or if you have a lag in external rotation. Start with kneeling jammer to build to overhead pressing. It is important to do the small stuff to feed in to these exercises.
12 weeks
Some of the common deficits seen at the 12 week mark tend to be pushing in the horizontal plane, particularly in the eccentric strength phase.
Return to sport criteria – shoulders are a bit behind the work being done in the lower limb.
There are lots of things that can be looked at around returning to play but Edel dove in to what is being looked at at the Sport Surgery Clinic

Rotational strength: Rotator cuff strength interlimb asymmetry
External rotation / internal rotation strength ratio imbalance (Adhern 2016). There are so many different ways to measure rotational strength and so many different tools with most of the research predominantly being in overhead athletes. Edel showed some of the findings from her work with contact athletes and highlighted the tools used to assess this will have an impact on the strength ratio imbalances and % bodyweight numbers you will see.

In Edel’s clinical and research experience it is rare that peak torque is down.
Often end range external rotation is down with the greatest deficit in the inner range posterior cuff.
It is important to take measurements throughout range as seen below.

The graph above shows the % bodyweight numbers for peak torque through various ranges.
The internal rotators are a bigger muscle group which tends to be stronger than the external rotations except in the inner range internal rotation (-50°).

Explosive strength & power testing:
Countermovement Push Up

The arrows in the video represent the vertical ground reaction forces.

You can see the athlete off-loading on to plate one during the eccentric deceleration phase. During the eccentric deceleration phase is where you tend to see biggest deficit throughout the push jump.
These are players that are going back to high load demanding environments and we should be ticking all these boxes as these are trainable and modifiable factors.
In non-injured athletes there may be a 10% difference between left to right. This athlete had about a 40% difference in the deceleration phase.
Concentric Push Up

You can see during the concentric phase the goalkeeper favours plate 1, his unoperated side.
Box drop land
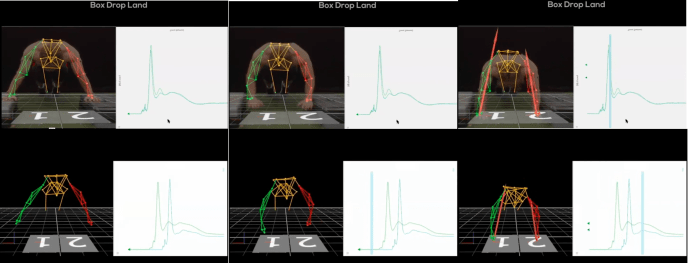
Looking at peak landing force throughout this test.
You can see the rugby athlete favouring his right side during the landing.
If you just look at just peak force you can see it is actually greater on the operated side. You have to look at the whole data. Look at kinematics over time.
They are currently looking at a pathological cohort to see if having these deficits are prognostics in any way to re-injury or persistent pain.
Edel presented some normative values from her PhD work as well as some correlations between the push up tests and isokinetic testing which will hopefully be published soon so keep an eye out for this.
Physical and psychological readiness are both important in the return to play process.
- Important to have set objective markers – lets the athlete see they are achieving markers before returning back to play.
- Expectation management – players often have unrealistic expectations.
- Clinicians often overestimate the expected outcomes.
- It is hard to tick all the boxes and get players through in 12 – 14 weeks.
A shoulder dislocation will have a similar psychological impact as an ACL injury.
Tweet
There is a difference between sending players back to play vs sending players back having ticked all the boxes.
Tweet
Players have gone back to play with strength and proprioceptive deficits that can last up to two years.
There can be complications if the surgeon finds a rotator cuff tear or performs a bicep tenotomy. It is a completely different ball game if the dynamic structures are affected as you would be looking at a minimum 6 month return with a rotator cuff repair.
Edel has also had a review published looking at outcome measures post shoulder stabilisation from 62 articles in the athletic cohort with the mean return to sport times shown below.

You can also check out more of Edel’s great work here: https://sportssurgeryclinic.com/management-shoulder-dislocation-instability-gaa-edel-fanning/ and here: https://sportsmap.com.au/podcast/12-return-to-play-for-shoulder-injuries-in-collision-based-sports-with-edel-fanning/
7,327 views
1 thought on “The Young Contact Athlete Post Latarjet”